
The current outbreak of monkeypox infections since January has brought up new concerns. Two of these new concerns are that the disease is more prevalent among males (99% of cases with available gender details), and the majority of cases are transmitted by men having sex with men (MSM). The MSM link was reported in 97% of cases with sexual orientation details, according to the World Health Organisation (WHO).
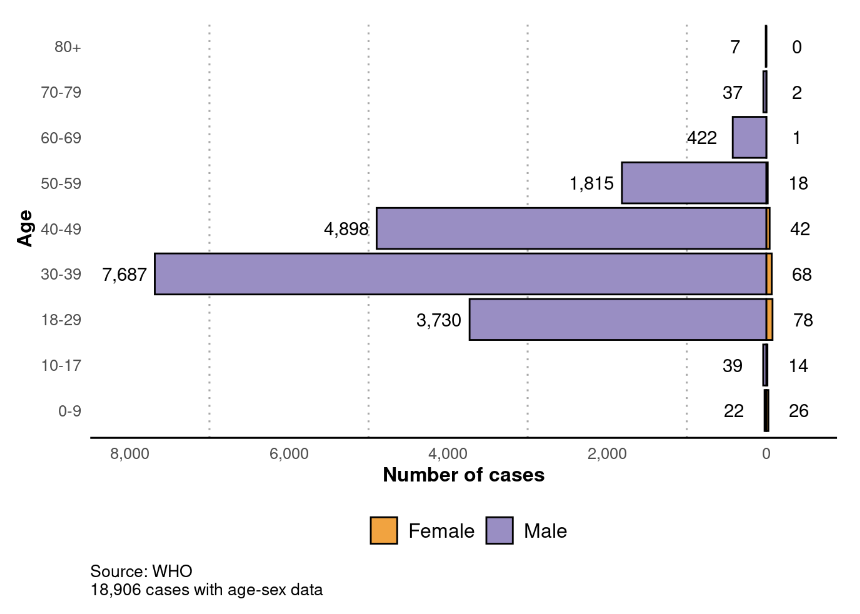
Age-Sex Distribution of Monkeypox Cases
In Nigeria, the disease is also prevalent among males. According to the Nigerian Centre for Disease Control (NCDC), 71% of all confirmed monkeypox cases in Nigeria were men, though the sexual orientation of the affected males in Nigeria and Africa has not been confirmed. Meanwhile, for all diseases captured by the NCDC, the prevalence among men was just 52%.
Ordinarily, “Monkeypox is a rare viral zoonotic infectious disease (i.e. an infection transmitted from animals to humans) that occurs sporadically, primarily in remote villages of Central and West Africa, near tropical rainforests.
Monkeypox is usually self-limiting, with symptoms lasting between 2 and 3 weeks. Severe cases occur more commonly among children, who also have greater mortality – the case fatality has ranged from 1% to 10%, higher in Congo Basin cases”, according to the NCDC.
The World Health Organisation also warned that, “Although most cases in current outbreaks have presented with mild disease symptoms, monkeypox virus (MPXV) may cause severe disease in certain population groups (young children, pregnant women, immunosuppressed persons)”
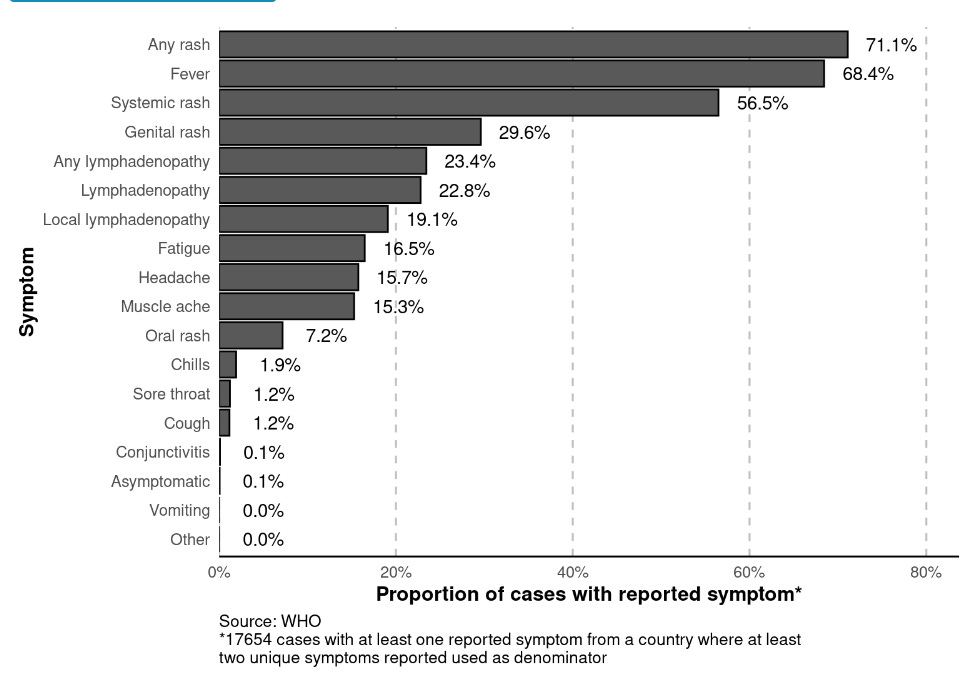
The most commonly reported symptom is “any rash” and is reported in 71% of cases with at least one reported symptom. “Any rash refers to one or more rash symptoms (systemic, oral, genital, or unknown location), and “any lymphadenopathy” refers to either general or local lymphadenopathy, the World’s health body clarified.
Reported Symptoms of Monkeypox
However, just as MSM are now linked to high incidence of monkeypox infection and transmission, studies in Nigeria show a similar higher risk of HIV and other sexually transmitted diseasess among MSM in Abuja and Lagos. Thus, there may be a need to intervene in the monkeypox spread in Nigeria by concentrating care efforts also on MSM in Nigeria.

Nigeria has recorded 157 new monkeypox infections, the highest in West Africa as of 10 August 2022, since the recent outbreak of the disease in January. This figure adds up the country’s all-time monkeypox cases to 2,131, also the highest in West Africa.
Within the same period, West and Central Africa recorded 335 confirmed new monkeypox cases and 6 deaths from the disease. These represent 1% and 50% of global cases and deaths, respectively.
Globally, 31,665 confirmed cases and 150 probable cases, including 12 deaths, have been reported to WHO between 1 January 2022 and August 10, 2022.
Beyond Nigeria, the Democratic Republic of the Congo has the highest number of all-time cases (2,618) and new infections (163) in West and Central Africa combined. This high incidence in DRC and Nigeria calls for concern when WHO considers the confirmation of one case of monkeypox in a country as an outbreak.
For this reason, the WHO Director-General, Dr Tedros Ghebreyesus has designated the 2022 outbreak “a public health emergency of international concern” and issued temporary recommendations about the outbreak.

While WHO assesses the global risk as “Moderate”, it discerned high, moderate, and low moderate degrees of risk in the various world regions.
Europe, with the highest case total of 18,005 monkeypox infections, is the only region designated as high risk even though it has the least case fatality risk of 0.01% if the Western Pacific and East Mediterranean Regions, which recorded no fatalities at all, are not considered.
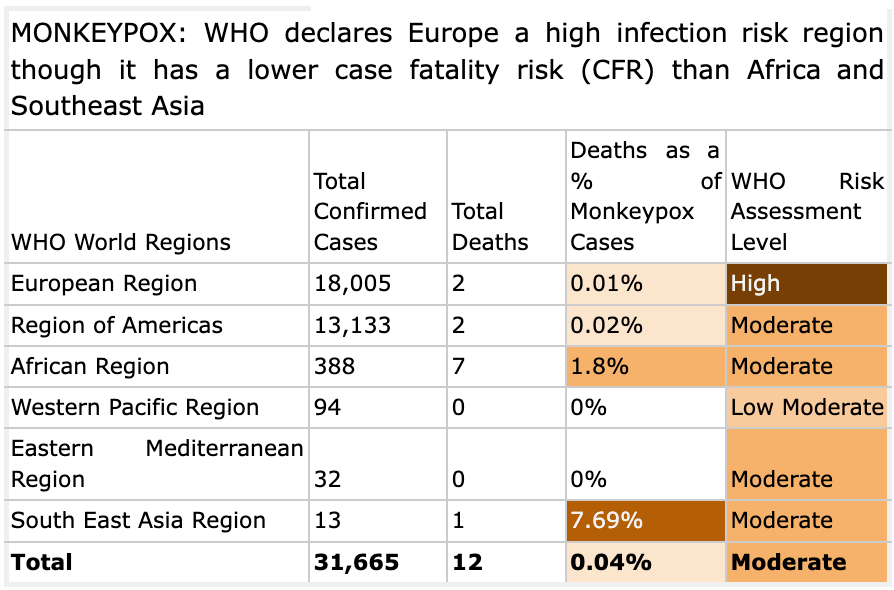
The South East Asia Region had the highest case fatality risk of 1 death in 13 cases (7.69%), followed by the Africa Region with 7 deaths in 388 cases (1.8%). The WHO designated the Western Pacific Region as the only Low Moderate risk region. The remaining 4 regions (African Region, Region of the Americas, Eastern Mediterranean Region and the South-East Asia Region) were designated regions of Moderate Risk.
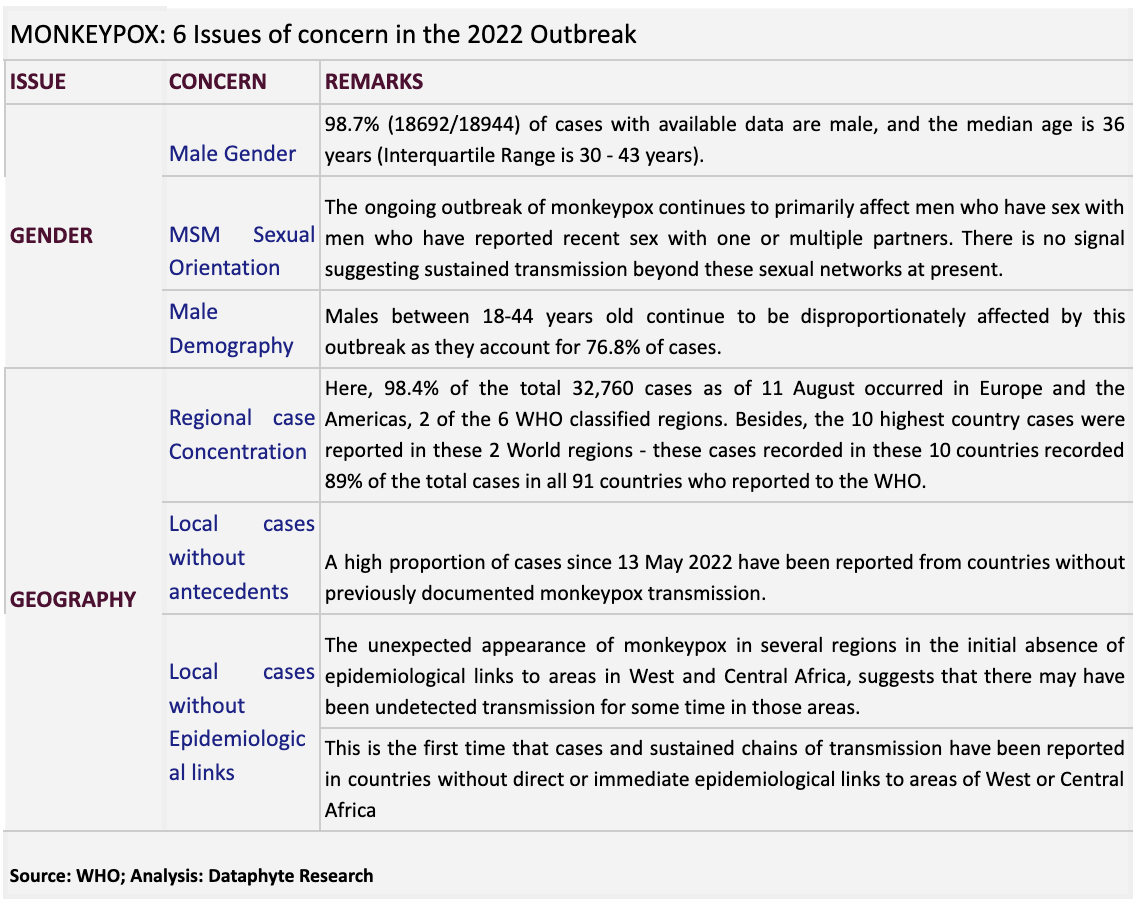
The 2 Broad Issues and 6 Concerns about this Outbreak
Two striking features of the 2022 monkeypox outbreak are its prevalence along geographic and gender lines. Relating to geography, Europe and the Americas reported 98.4% of the 32,760 confirmed cases as of 11 August 2022. This has earned Europe a high risk region status by WHO.

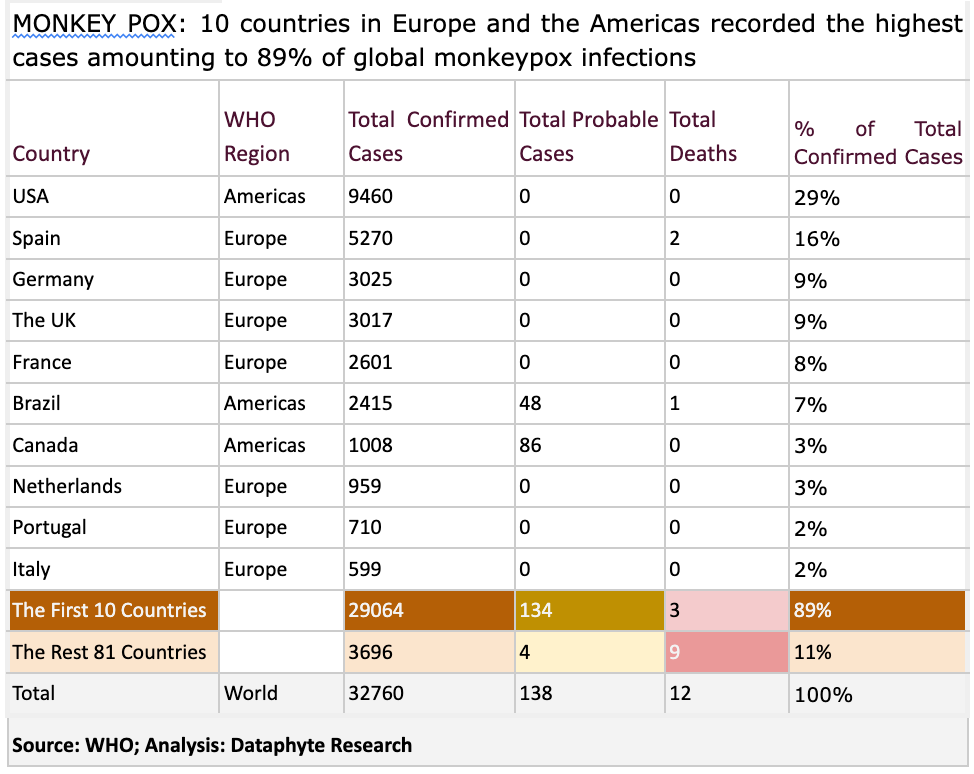
Likewise, the 10 countries with the highest confirmed monkeypox cases globally are all located in Europe and the Americas and together account for 89% of the 32,760 cases reported globally.
The countries are: The United States of America (8,902); Spain (5,162); Germany (3,025); The United Kingdom (3,017); France (2,423); Brazil (2,293); Canada (990); Netherlands (959); Portugal (710); and Italy (599).
MONKEY POX: 10 countries in Europe and the Americas recorded the highest cases amounting to 89% of global monkeypox infections
Beside the high incidence of the disease in Europe and the Americas, there is also the issue of gender. Here the prevalence of the disease is skewed toward males between 30 and 43 years and toward men who have sex with men (MSM).
The 2 Current Drivers of this Monkeypox Outbreak
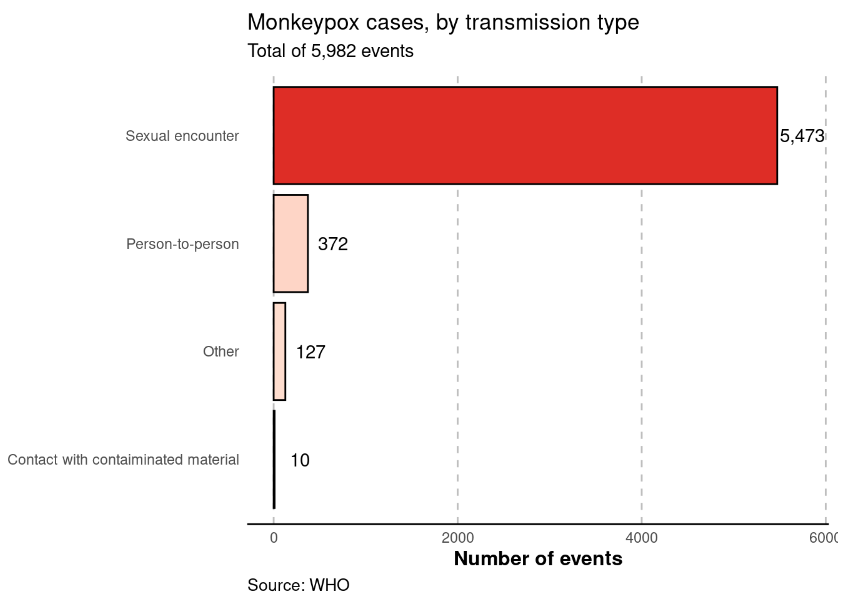
Sexual activity and sexual orientation are the 2 current drivers of Monkeypox infections and transmission globally. This has proven in both the types of transmission and types of exposure to the disease.
Of all reported types of transmission, a sexual encounter was reported most commonly, with 5,473 of 5,982 (91.5%) of all reported transmission events.
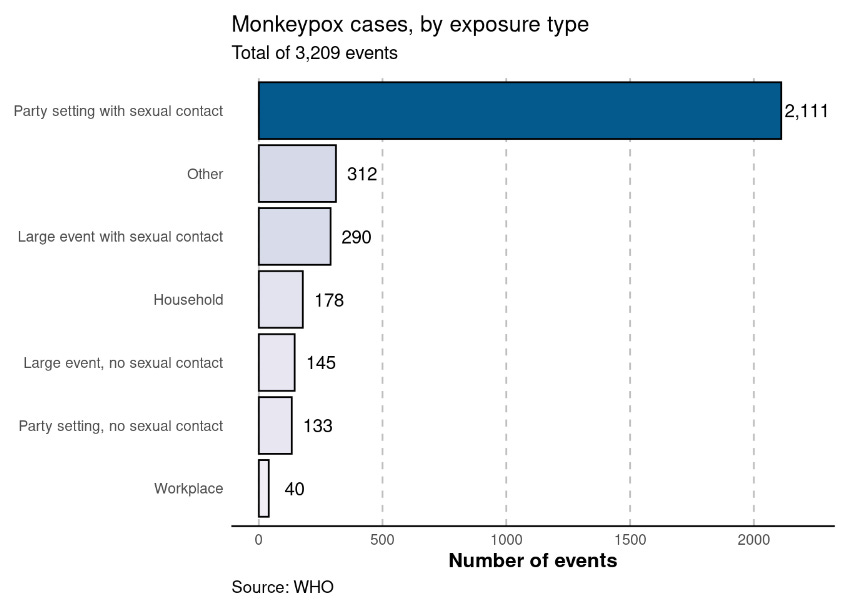
Of all settings in which cases were likely exposed, the most common was in party setting with sexual contacts, with 2,111 of 3,209 (65.8%) of all likely exposure categories.
91% of transmission of monkey pox is through sexual activity
Party setting with sexual contact exposes to monkeypox infection than party setting without sexual at the ratio of 16:1. Large event with sexual contact exposed people to monkeypox infection than large event without sexual contact by the ratio 2:1. Overall, sex in social gatherings account for 2,401 of 3209 events. Thus 75% of exposure was through sexual activity, making sex the major determinant of infection with monkeypox
As shown below, and stated previously, the ongoing outbreak is largely developing in men who have sex with men (defined as homosexual or bisexual males in detailed case forms) networks. In the following analyses, we have re-coded men reported as bisexual as men who have sex with men. Note that reported sexual orientation does not necessarily reflect who the case has had recent sexual history with nor does it imply sexual activity. Generally, severity has been low, with few reported hospitalisations and deaths:
The need for MSM data for Monkeypox Control in Africa
The World Health Organisation has established that the 2 drivers of the current wave of monkeypox infections are sexual activity and sexual orientation. Thus, there is the need to examine and sensitise the sexually active African population on special social precautions they need to observe to prevent the disease.
- Among cases with known data on sexual orientation, 97.2% (8228/8466) identified as men who have sex with men. Of those identified as men who have sex with men, 62/8228 (0.8%) were identified as bisexual men.
- Among those with known HIV status 38.5% (3,425/8,905) were HIV-positive. Note that information on HIV status is not available for the majority of cases, and for those for which it is available, it is likely to be skewed towards those reporting positive HIV results.
There is also the need to estimate the threats this disease poses to MSM to inform interventions that may be needed. Yet, studies have shown that without testing, men who have sex with men were not aware of their infection with chlamydia and gonorrhoea. Likewise they may not be aware of an asymptomatic monkeypox infection, thereby increasing the risk of transmission to their partners.
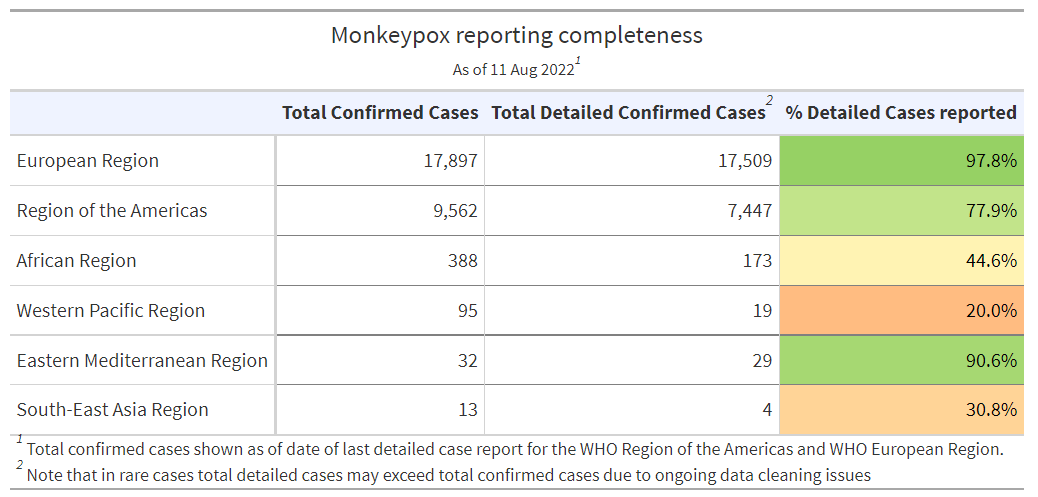
The African region gave less than half the required detail about people infected with monkeypox compared to Europe, the Eastern Mediterranean, and the Americas. With Africa coming third in the number of monkeypox infections and the second highest in case fatality risk, collating and reporting details of cases would be helpful to control further transmission and provide knowledge to combat future outbreaks.
While monkeypox transmission has not been traced directly to a particular sexual behaviour or sexual activity in Nigeria and Africa as a whole, the high incidence of transmission and exposure reported with sexual activity and among men who have sex with men in Europe and the Americas calls for concerted efforts to prevent a repeat of such episodes among MSM in Nigeria.
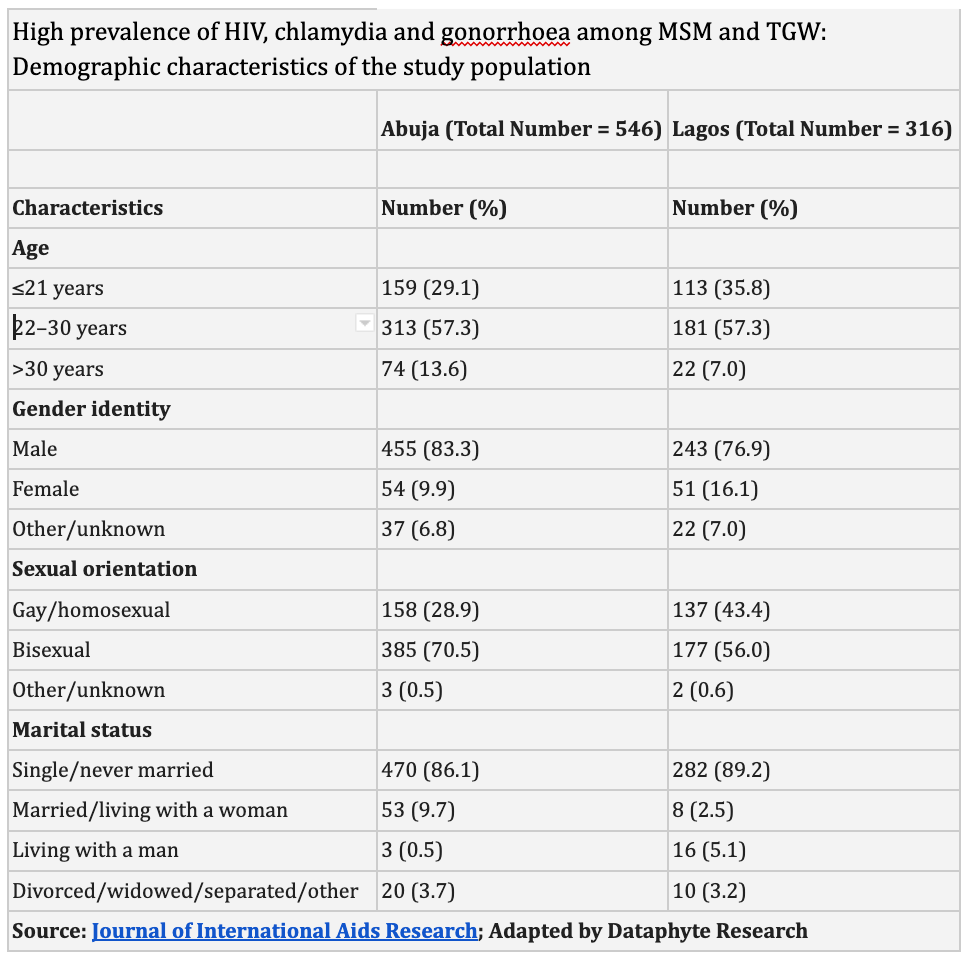
Several studies in Nigeria have shown that men who have sex with men (MSM) and transgender women (TGW) face higher risks of infection and transmission of diseases such as chlamydia, gonorrhoea and HIV than those with heterosexual behaviours.
“The RDS-weighted prevalence of HIV among MSM and TGW in Abuja is more than 10 times the reported prevalence of 3.4% in the general Nigerian population. The RDS-weighted prevalence of HIV among MSM and TGW in Lagos is even higher.”
This was revealed in the paper, “High prevalence of HIV, chlamydia and gonorrhoea among men who have sex with men and transgender women attending trusted community centres in Abuja and Lagos, Nigeria.”
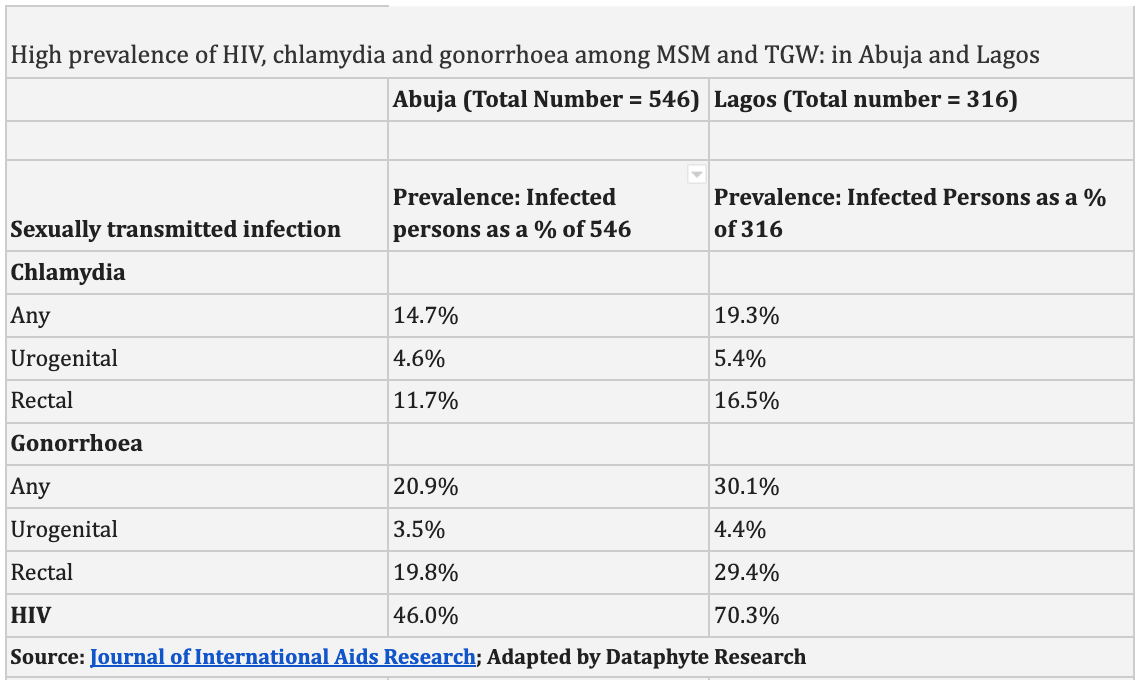
On the prevalence of other STIs among MSM, the authors declared: “The prevalence of both chlamydia and gonorrhoea is higher in our study than the 4.2% prevalence of both infections among MSM in Lagos reported in an earlier unpublished report that used voluntary screening with urethral swabs or syndromic diagnosis. Universal screening programmes deployed in Tanzania, Botswana and Kenya have reported similarly high STI prevalence rates of between 12 and 20% in a relatively young population.
The authors discovered “a high burden of infection with HIV and asymptomatic chlamydia and gonorrhoea among MSM and TGW in Nigeria.” They argued further that, “Most chlamydia and gonorrhoea cases would have been missed without anorectal screening, which might only occur upon disclosure of MSM status to a health care provider. Such disclosure was exceedingly uncommon among participants prior to enrolment in this cohort.”
Thus, the screening of groups in Nigeria and Africa that are vulnerable to the disease, like MSM and TGW may help in the control of monkeypox too, going by the strong link between this type of sexual behaviour and the transmission of the disease. However, it is difficult to convince people of such voluntary screening because it presuposses a disclosure of the person’s sexual orientation.
To this, Babajide Keshinro and his colleagues suggested then that MSM-focused, trusted community health centres may be used as a model of care to facilitate this disclosure and provide health care services that meet the unique needs of the MSM and TGW in Nigeria.
Treatment, Infection Prevention and Control
The NCDC diseases factsheet clarifies that there are no specific treatments available for monkeypox infection, although various novel antivirals have in-vitro and animal data supportive of effect such as Brincindofovir and Tecovirimat.
However, vaccination against smallpox has been proven to be 85% effective in preventing monkeypox but is no longer routinely available following global smallpox eradication. Post exposure vaccination may help prevent the disease or reduce its severity.
Also, prior smallpox vaccination will likely result in having a milder disease course. Screening and management of co-morbidities and all other secondary infections should be carried out.
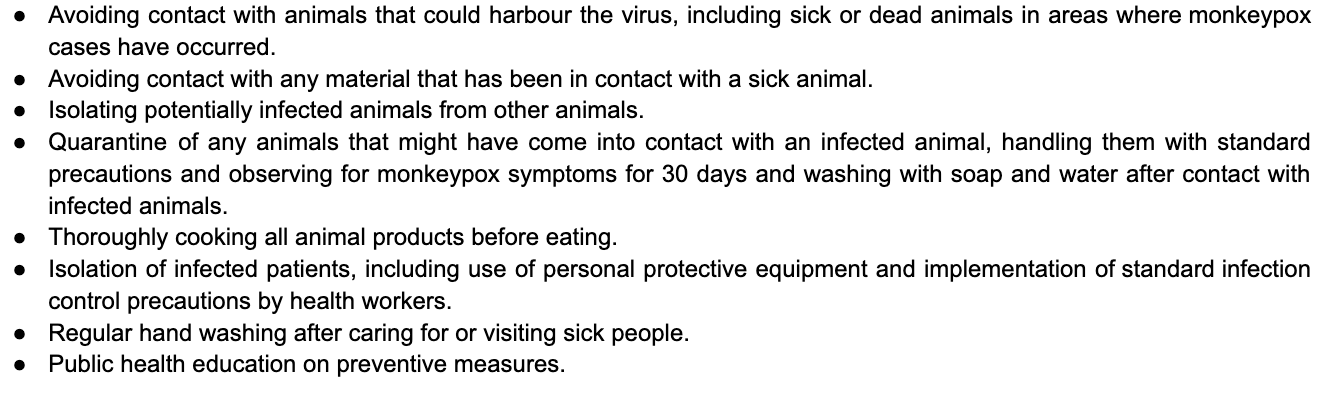
However, the Disease Control Agency has listed the following guidelines on prevention and control:
Meanwhile, the Nigeria Centre for Disease Control, NCDC situation report on Monday showed that the confirmed and suspected cases of monkeypox recorded in Nigeria are yet to abate.
“From January 1 to July 31, 2022, there have now been 413 suspected cases and 157 confirmed cases (105 male, 52 female) from 26 states – Lagos (20), Ondo (14), Adamawa (13), Delta (12), Bayelsa (12), Rivers (11), Edo (8), Nasarawa (8), Plateau (6), Anambra (6), FCT (5), Taraba (5), Kwara (5), Kano (5), Imo (4), Cross River (3), Borno (3), Oyo (3), Abia (3), Gombe (3), Katsina (2), Kogi (2), Niger (1), Ogun (1), Bauchi (1) and Akwa Ibom (1).
Lagos still reports the highest monkeypox cases of 20, while 4 deaths were recorded from 4 states – Delta (1), Lagos (1), Ondo (1) and Akwa Ibom (1).
“Overall, since the re-emergence of Monkeypox in September 2017 and to July 31, 2022, a total of 925 suspected cases have been reported from 35 states in the country.”
Taking personal precautions as the NCDC advised may be the first step towards subduing the current outbreak across the country.
Dataphyte
